👶 Pediatric Ideal Body Weight Calculator
Estimate ideal body weight for children & adolescents using age, height & gender — based on CDC growth standards
| Age | Boys Weight (kg) | Boys Height (cm) | Girls Weight (kg) | Girls Height (cm) |
|---|---|---|---|---|
| Birth | 3.5 | 49.9 | 3.4 | 49.1 |
| 6 months | 7.9 | 67.6 | 7.3 | 65.7 |
| 1 year | 10.2 | 75.7 | 9.5 | 74.0 |
| 2 years | 12.3 | 87.1 | 11.8 | 86.0 |
| 3 years | 14.3 | 95.0 | 13.9 | 94.1 |
| 4 years | 16.3 | 102.9 | 16.1 | 101.6 |
| 5 years | 18.3 | 109.9 | 17.7 | 108.4 |
| 6 years | 20.7 | 116.1 | 19.5 | 114.6 |
| 7 years | 22.9 | 121.7 | 21.8 | 120.1 |
| 8 years | 25.6 | 127.0 | 24.8 | 125.4 |
| 9 years | 28.6 | 132.2 | 28.5 | 130.7 |
| 10 years | 31.9 | 137.5 | 32.5 | 136.5 |
| 12 years | 40.7 | 149.1 | 41.5 | 151.5 |
| 14 years | 52.1 | 163.8 | 50.3 | 159.5 |
| 16 years | 62.1 | 173.4 | 53.5 | 162.5 |
| 18 years | 68.0 | 177.0 | 56.7 | 163.7 |
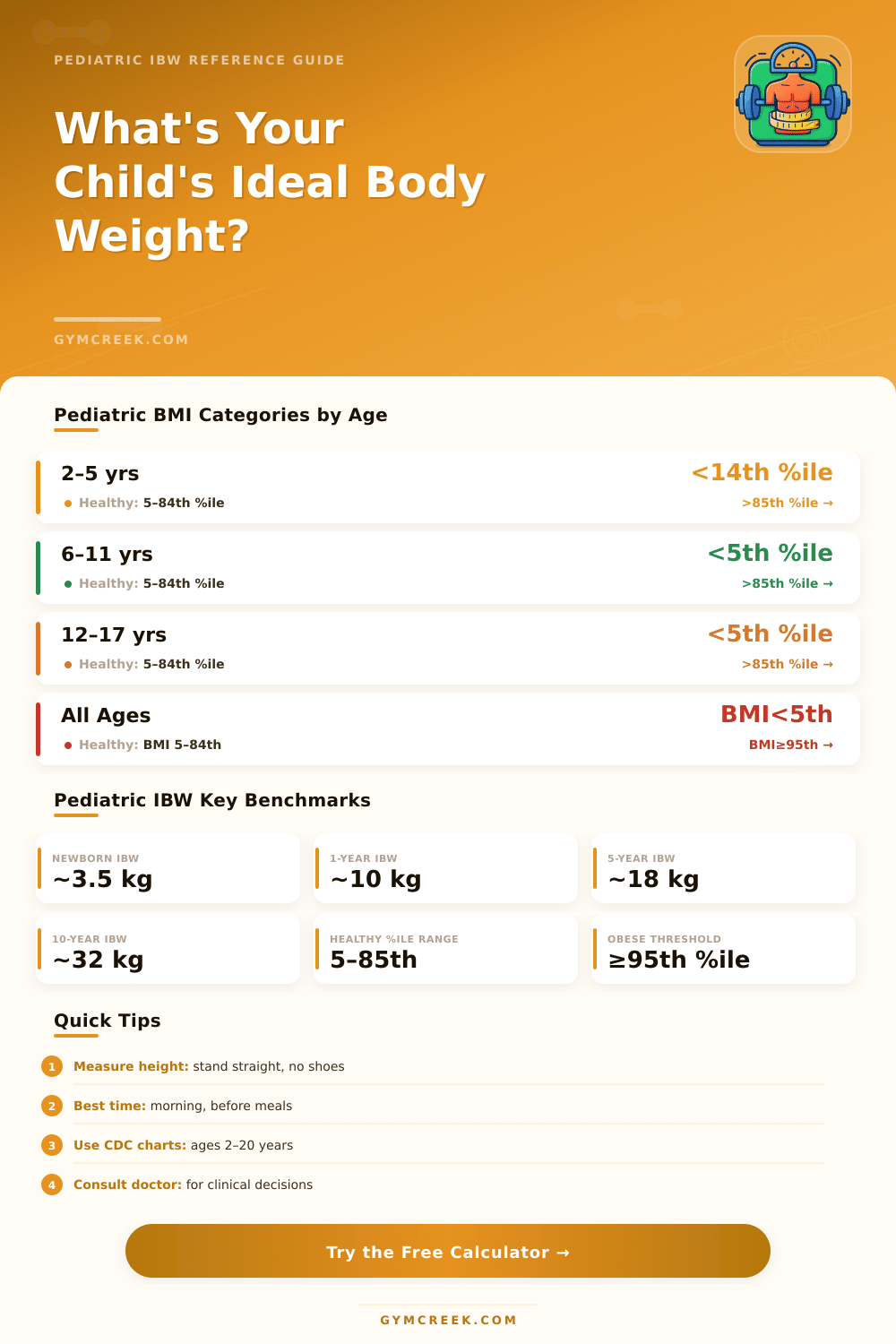
| BMI Percentile | Weight Status | Action Recommended | Clinical Note |
|---|---|---|---|
| Below 5th | Underweight | Nutritional assessment | Evaluate for underlying causes |
| 5th – 84th | Healthy Weight | Maintain healthy habits | Normal range for age/gender |
| 85th – 94th | Overweight | Lifestyle counseling | Monitor weight trends |
| 95th or above | Obese | Medical evaluation | Assess comorbidities |
| 120% of 95th | Severe Obesity | Specialist referral | Multidisciplinary care needed |
| Formula / Method | Age Range | Basis | Notes |
|---|---|---|---|
| McLaren / CDC 50th %ile | 0–20 years | Height-for-age 50th %ile weight | Most clinically used |
| Traub & Johnson | 1–17 years | Height-based equation | Good for drug dosing |
| Devine (adapted) | 12–18 years | Adult formula adjusted | Less accurate for young children |
| BMI-based (CDC 50th) | 2–20 years | 50th %ile BMI x height² | Standard clinical approach |
| Weight-for-height %ile | 0–2 years | WHO growth standards | Used for infants and toddlers |
• Children grow at different rates — short-term deviations from IBW are often normal.
• Growth velocity (trend over time) is more important than a single measurement.
• BMI-for-age percentiles, not absolute BMI values, are used for children and teens.
• This calculator uses CDC 50th percentile weight-for-height as the IBW reference standard.
Figuring out the right Body Weight for children is not easy, in medicine there is real debate about what makes the “ideal” numbers or how to measure them. That causes real headache for both Pediatrics doctors and parents who try to figure that out.
The ideal Body Weight, or IBW, has big importance for how one treats children. Doctors commonly depend on it to control growth, figure out doses of medicines and judge the general shape. Getting it right matters a lot especially for medicines like acyclovir, digoxin and morphine, where exactness is key.
Finding the Right Body Weight for Children
Being wrong about IBW can create serious troubles. For instance, for an obese child, if one tries to dose medicine according to his real weight, which does not account for the fat amount, one risks to give too much, which is really dangerous.
There are at least three mainstream ways to count IBW for children. The methods of McLaren, Moore and that based on BMI are the most known. One of them starts form the thought, that the ideal weight should match the same percentile as the height of the child, so, if the height of a child is in the 95th percentile, one chooses the weight in that same 95th percentile for its age as target.
Some specialists also apply the formula of Devine. When children suffer because of obesity, another way is made up of using diet references, that is set to BMI for age in exactly the 50th percentile.
This is where things get complicated: various methods deliver entirely different results. Almost all approaches give values, that statistically differ from that of McLaren, if one compares them directly. The differences grow a lot at extreme spots.
Especially for really high or low percentiles of height, and they expand as children mature. The fact is, that their still lacks a gold standard for exactly setting IBW in children.
BMI commonly appears as a tool for screening. The math is simple: weight in kilos divided by square of height in metres. For children and youngsters of two until nineteen years, doctors use percentiles of BMI for age, taken from growth charts of CDC.
Even so, BMI has clear limits. A child can reach high value only because of big physical build or strong muscles, not because of extra fat. Rather, a child with little build can have normal BMI, although it carries too much body fat.
During puberty it becomes even more confusing, when fast weight gain is quite a lot normal.
Having reliable ratings of IBW helps to explain, whether children improve and if the therapy really works. It gives also to families a target for action. The truth is to keep enough fat and muscle reserves, so that a child can rush to recover after surgery or resist common diseases without getting weak.
Diet plays a clear role, too much processed junk and lack of balanced nutrition push the weight to extra fat. Genetics also matter, because some folks inherit a trend to gainheavy more easily or own slower metabolisms.